


Unusual COVID-19 facts - Over 50% of hospitalisations have hypertension


This data was taken from the CDC analysis of hospitalisations and mortality between March 2020 and March 2021. Quote from paper - “540,667 (11.0%) were patients with COVID-19, of whom 94.9% had at least 1 underlying medical condition. Essential hypertension (50.4%), disorders of lipid metabolism (49.4%), and obesity (33.0%) were the most common.”
Gundlapalli, M. D. "Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021."
Hypertension is not usually associated with increased severity of symptoms or death in any other infection. There is no doubt that this is very unique to COVID-19.
There is no increased risk of catching SARS-COV2 if you are hypertensive. It is just the risk of severe disease once infected.
It was the first observation I made in March 2020 with the data coming out of China, where over 76% of hospitalisations had a diagnosis of hypertension and there were only a few children affected. It caused me to look for any factor that could account for those differences.
During this research I came across serum (free) ACE-2 being elevated in hypertension. It seemed important but I could not see the link at the time. Normally ACE-2 is attached to cells lining blood vessels (endothelial cells) and a small fraction is free floating in healthy individuals.
The picture below shows a cross section of a blood vessel with pinkish red endothelial cells lining the vessel and pink blood in the middle. The special ACE-2 snipping enzyme is ADAM-17 leading to increased levels of serum (free) ACE-2.

McMillan, Philip, et al. "COVID-19—A theory of autoimmunity against ACE-2 explained." Frontiers in Immunology 12 (2021): 582166.
In certain conditions, the serum ACE-2 fraction increases in the blood stream. This is related to gender, specific comorbidities (like diabetes, hypertension, obesity…) and as people get older.
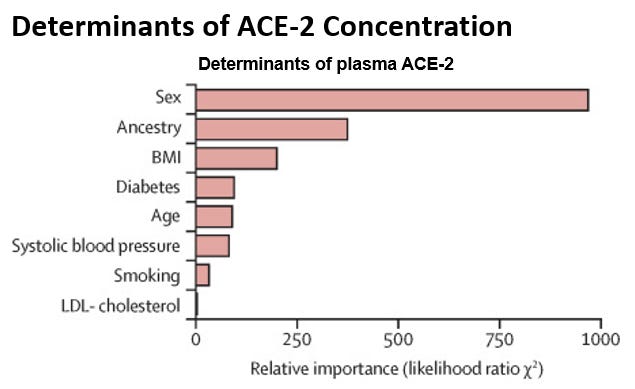
Narula, Sukrit, et al. "Plasma ACE2 and risk of death or cardiometabolic diseases: a case-cohort analysis." The Lancet 396.10256 (2020): 968-976.
Since ACE-2 is the entry receptor for SARS-COV2 and binds tightly to the viral spike protein, could it be relevant to the severity of COVID-19?
This question was the dominant focus which eventually led me to autoimmunity to ACE-2 as the primary mechanism for the cytokine storm (immune dysregulation).
Look out for more posts as I bring you along my research journey.
Absolutely – ACE2 dysregulation is a cause of severity of Covid-19. Once bound to S protein ACE2 is not able to fulfil its main function in renin angiotensin system (RAS) – regulation of blood pressure and inflammatory processes. ACE2 is more abundant and with lower affinity in children, therefore, SC2 infection may not cause significant dysregulation or the RAS. In old adults and seniors expression of AC2 on cell surfaces is less evident but with higher affinity, therefore, anything binding to ACE2 decreased number of functioning ACE2 that leads to increased risk of myocardial fibrosis, inflammation and cardiovascular disease.
due to 5X increase in ace 2 from ace and arb drugs?