

Every time we think we’ve unraveled the complexities of the immune response to COVID-19 vaccines, new data emerges that forces a reevaluation. This week, a new study published on July 16th, 2025, did exactly that—highlighting a striking difference between the Pfizer (BNT162b2) and Moderna (mRNA-1273) vaccines in how they influence antibody class switching.
Once again, the focus is on IgG4—an antibody subclass typically associated with immune tolerance, not immune activation. We see IgG4 in beekeepers, for instance, who develop tolerance after repeated stings. It’s a protective adaptation that prevents overreaction to repeated exposure. But what happens when that tolerance mechanism is applied to a virus like SARS-CoV-2, which the body needs to clear, not ignore?
The Study’s Findings: Pfizer Induces More IgG4
This latest research compared immune responses in individuals boosted with either Pfizer or Moderna. The key finding?
Both vaccines induced IgG4, but Pfizer did so more significantly.
That surprised many of us. Moderna uses more mRNA (100 µg vs. Pfizer's 30 µg)—so logically, one might expect it to cause more immune tolerance. But it didn’t. The IgG4 response was markedly higher in the Pfizer group.
So why would a lower-dose vaccine lead to more immune tolerance?
Siebner, Alex S., et al. "Class switch towards IgG2 and IgG4 is more pronounced in BNT162b2 compared to mRNA-1273 COVID-19 vaccinees." International Journal of Infectious Diseases.
The Molecular Detail That May Hold the Answer
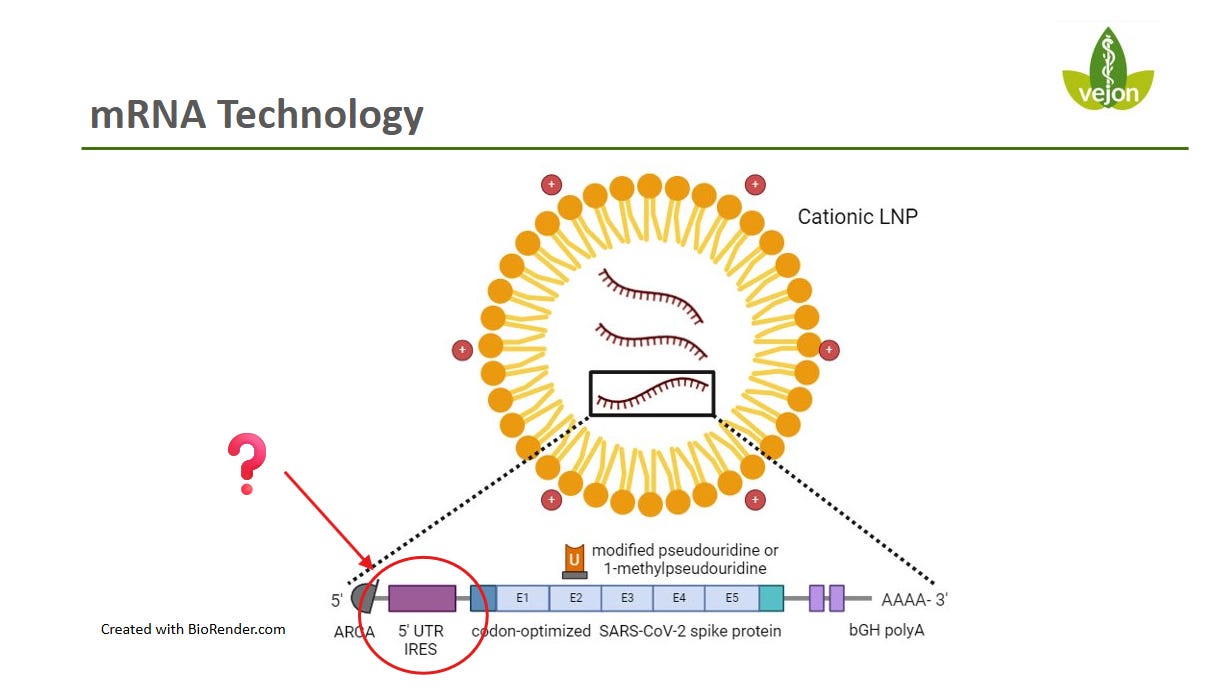
Digging deeper into the vaccine design reveals a crucial difference: the 5′ untranslated region (UTR) of the mRNA.
Pfizer uses a globin-derived UTR—a sequence originally from human hemoglobin mRNA, chosen for its stability and efficient translation.
Moderna, in contrast, uses a proprietary UTR optimized for strong immune activation.
This 5′ UTR acts as a “start signal” for the ribosome, guiding how spike protein is produced. The theory is that Pfizer’s globin UTR enables longer-lasting, lower-intensity spike protein expression. Over time, this prolonged exposure may nudge the immune system into a tolerogenic state, increasing IgG4 production.
It’s a small molecular detail—but one with large immunological consequences.
Why Does This Matter?
Earlier studies have already shown that repeated mRNA vaccination can lead to IgG4 making up as much as 45% of the antibody profile, compared to just 1% after natural infection. This latest paper adds that Pfizer’s formulation may be driving this shift even more strongly than Moderna’s.
One study even found that elevated IgG4 levels were associated with an 80% relative increase in breakthrough infection risk.
Why? Because IgG4 is non-inflammatory. It blocks rather than destroys. Your immune system stops treating the spike protein as a threat—and starts tolerating it.
Could Spike Protein Persist as a Result?
That leads to the next question: If the body becomes tolerant, could the spike protein linger?
A growing body of data suggests that in some individuals, spike protein can still be detected in the blood nearly two years after vaccination. This isn't true for everyone—but it's true for enough people to raise serious concerns.
The implication is that Pfizer’s vaccine design may be promoting a form of long-term antigen exposure, coupled with a muted immune response. That’s a setup for chronic immune confusion—or worse, immune exhaustion.
Why Wasn’t This Taken More Seriously in 2022?
This isn’t a new issue. The possibility of IgG4 class switching was flagged as early as 2022. The scientific community knew. The data was there. But the issue was largely ignored, dismissed as unimportant.
Now, in hindsight, we’re seeing that it was anything but minor. When nearly half of your antibody response shifts to a subclass associated with immune tolerance, we should be asking hard questions.
And yet—we’re not.
Where Do We Go From Here?
We need to:
Re-examine vaccine platform differences with fresh eyes.
Investigate long-term immune effects, especially IgG subclass profiles.
Ask why regulatory and scientific bodies didn’t respond more proactively to early warning signs.
This is not about blame—it’s about responsibility and scientific rigor. We must remain open to the possibility that the tools we thought were flawless may require adjustment.
Final Thoughts
Immune tolerance was never the intended outcome of mass vaccination. Yet, through design choices like the globin UTR, we may have inadvertently moved the immune system in that direction—at least in some individuals.
And that means we need to adjust our thinking—and our strategies.
The science is still unfolding. But one thing is clear:
We can’t fix what we refuse to investigate.
The truth lives in the uncomfortable questions.
Vejon COVID-19 Review is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
