


Beware of the eye of the COVID-19 pandemic hurricane


Why do I define this period as the eye of the hurricane?
The eye of a hurricane is very disconcerting to experience, as the winds settle, and the sun comes out.
The reason there is such devastation where the hurricane eye passes over, is that the winds change to the opposite direction and start at 150 miles per hour over a few minutes. Any tree that managed to cope is then blown away.
There is a pandemic lull at present and it is not clear if the pandemic has now passed or we are temporarily in the eye of the hurricane.
If there is no change in an hour (in a few months), then the hurricane has probably passed.
There is an appearance of calm and it seems that the worst is behind us. Omicron is not causing severe respiratory lung disease as frequently and the ITU beds remain available.
However, infection levels remain elevated across the population in highly vaccinated regions of the world. This suggests that natural mucosal immunity is likely to be impaired as evidenced with health care workers after vaccination.

What could happen next?
Excess mortality is already elevated but primarily for non-covid deaths, which gives the impression that they are unrelated. My research into COVID-19 autoimmunity predicts that immune priming with spike protein (through infection or vaccination) can lead to chronic autoimmune responses with associated thromboembolic complications.

Therefore, as virus continues to circulate into the autumn period, and vitamin D levels fall, there will be an upsurge in clots of all forms (DVT’s, PE’s, heart attacks, stroke).
Additionally, BA2.75 will increase in circulation with increased lung pathology and place direct pressure on health systems. Note that BA2.75 levels are just starting to rise in Europe and North America. Japan is currently having the worst COVID-19 outcomes since the start of the pandemic. Seems to coincide with increased spread of BA2.75.

Credit: Eric Topol - Twitter
This time, the health care workers will not be willing to face the pandemic alone and chronic sickness will further impair response. Once staffing numbers fall below a threshold, the burnout for remaining members of staff increases rapidly.

As staff numbers decrease and patient load increases, standard urgent care will suffer and there is limited ability to respond to the frail elderly population.
Mortality will significantly increase in the over 70s and those with underlying comorbidities at risk for thromboembolic disease (diabetes, heart disease, hypertension, obesity). Primarily through an inability to treat in a timely fashion for these complex patients.
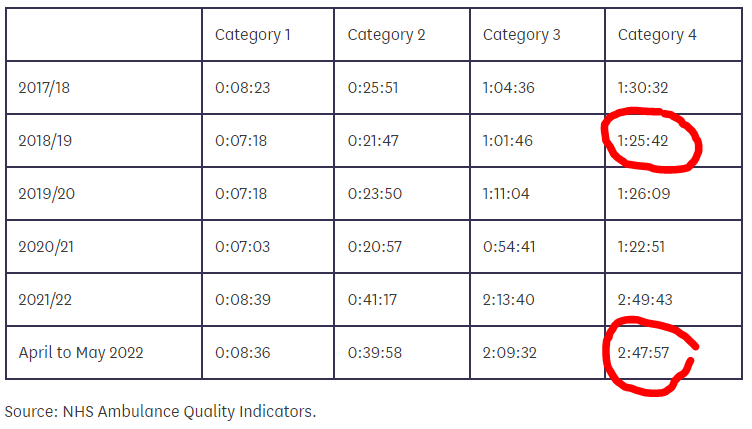
Ambulance response times increase exponentially with the increased mortality and morbidity for patients that need urgent treatment.
That could be you or your loved ones.
.This is likely to be a very difficult winter.
Do you have specific info on how the newest variant is affecting the populations in which it is currently prevalent like India? Thank you, Dr. M!